
Breastfeeding care after a cesarean section
When providing breastfeeding care after a cesarean section, healthcare professionals have to take into account a series of factors that have an impact on lactation.
It is known that women who give birth by C-section have lower breastfeeding rates at discharge and weeks thereafter than those who have had a vaginal birth. In addition, certain myths about cesarean births can make breastfeeding even more difficult.
Evidence suggests that the vast majority of difficulties with breastfeeding after a C-section are due to myths and inappropriate clinical practices.
If birth is expected to be a cesarean, the mother should have all the necessary information to be able to prepare herself as well as possible, especially if she desires to breastfeed her baby.
Prepare for breastfeeding
In all cases, information on infant feeding and breastfeeding is necessary to successfully initiate breastfeeding.
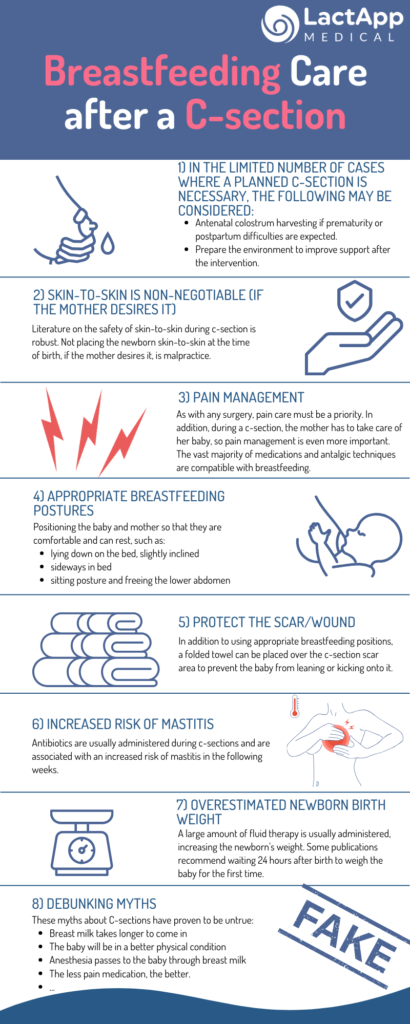
In cases when the C-section happens in a context in which an increased risk of hypogalactia is foreseen for other reasons (such as preterm birth, Intrauterine Growth Restriction (IUGR), preeclampsia, gestational diabetes, PCOS, and so on), the possibility of performing colostrum harvesting can be considered. This technique allows obtaining a certain amount of colostrum before birth, and possibly the most valuable about it is that it allows the woman to know her mammary gland and to have mastered the breast expression technique before giving birth.
It is also important to prepare the surroundings so that the mother receives the necessary support after the C-section.
Skin-to-skin
Some studies point out that there could be a delay of lactogenesis II after a C-section, but the cause of this delay could be due to the separation of the baby at birth and enabling skin-to-skin with the partner instead of the mother. Therefore, not enabling direct skin-to-skin of mother and baby during c-section can be considered an inadequate practice.
Pain management
The pain relief measures should be appropriate to ensure the minimum surgical wound.
Proper positioning
The mother’s comfort takes priority; also, look for antalgic positions, as well as positions for the baby that do not impact the scar.
Protecting the surgical wound
A very simple trick is to place a small folded towel at the area of the scar. In this way, the little kicks the baby could do with the feet, are felt less.
Early care for increased risk of mastitis
The use of antibiotics increases the risk of mastitis, so women who have had a baby by C-section could develop mastitis more easily. Therefore, we must provide these women with the necessary information so they can detect these difficulties in breastfeeding early.
Overestimated newborn birth weight
The infusion of intravenous fluids is related to an increase in the baby’s weight, so the baby’s weight after a C-section may be overestimated. An increasing number of publications recommend measuring newborn weight at 24h after cesarean section to avoid an overestimate.
Inform the mother and family
There are unfounded myths about breastfeeding after a cesarean section. The mother and people close to her should have access to accurate information and updated support to achieve the desired breastfeeding journey.
References
East CE, Dolan WJ, Forster DA. Antenatal breast milk expression by women with diabetes for improving infant outcomes. Cochrane Database of Systematic Reviews 2014, Issue 7. Art. No.: CD010408. DOI: 10.1002/14651858.CD010408.pub2. Accedida el 18 de abril de 2024.
Moore ER, Bergman N, Anderson GC, Medley N. Early skin‐to‐skin contact for mothers and their healthy newborn infants. Cochrane Database of Systematic Reviews 2016, Issue 11. Art. No.: CD003519. DOI: 10.1002/14651858.CD003519.pub4. Accedida el 18 de abril de 2024.